The Neural Metronome: The Science Behind Music and the Aging Brain
When we bring a live jazz set into a memory care community, we are not just playing music. Neuroscience research suggests that what we are doing can function as a meaningful health-supporting intervention, one that works through measurable pathways in the brain. This post summarizes what I found when I dug into the key research on rhythm, the aging brain, and why music may be one of the most accessible tools we have for supporting neurological health in older adults.
It is important to distinguish clinical music therapy, which is delivered by credentialed therapists using structured protocols, from community-based live music programs like ours. They are not the same thing. However, research suggests that music-based engagement, especially when it is consistent and social, can complement formal care in meaningful ways.
Your Brain Has a Beat
The basic idea behind all of this is neural entrainment. Every region of the brain produces electrical oscillations, rhythmic pulses of activity that scientists can measure with EEG. These oscillations are not random. They coordinate how different parts of the brain communicate. The motor cortex, which plans movement, often operates in the beta range of roughly 13 to 30 Hz. The auditory cortex responds to the frequency and timing structure of incoming sound.
When you hear a steady beat, neurons in the auditory cortex synchronize with it. Through connections in what neuroscientists call the auditory-motor pathway, this timing information influences the motor system. The brain adjusts its electrical firing patterns to match the tempo of the music. That is why people often tap their foot automatically. It is not a deliberate choice. It reflects how the brain is wired.
One helpful way to think about this is as a feedback loop in a robotics system. The auditory cortex functions as a sensor that detects an external timing signal. That signal feeds into thalamo-cortical circuitry, which continuously adjusts motor output to stay synchronized. The system runs automatically, much like a controller correcting a robot’s path without conscious decision-making.
I was surprised to learn that this pathway can remain relatively intact even when higher-order cognitive functions have deteriorated. That helps explain why someone with advanced dementia who can no longer hold a conversation may still clap along with a song. The rhythm reaches motor networks through neural routes that are less vulnerable than many language and memory systems.
What Happens When the Internal Clock Breaks
One of the most established clinical applications of this research is Rhythmic Auditory Stimulation, or RAS, developed largely by Dr. Michael Thaut and his colleagues.
To understand why it matters, consider Parkinson’s disease. Parkinson’s involves degeneration of neurons in the basal ganglia, a group of structures that plays a central role in timing and movement initiation. When this internal timing system is disrupted, patients can experience freezing of gait. They intend to walk, the motor cortex sends the signal, but the movement fails to initiate properly. This is one of the leading causes of falls and hospitalization in Parkinson’s patients.
RAS provides an external timing cue that can partially compensate for this deficit. A rhythmic signal delivered through music or a metronome travels from the ear to the auditory cortex and then to motor regions, helping organize movement timing through pathways that rely less heavily on the damaged basal ganglia. In one of Thaut’s earliest studies, patients who trained with RAS for three weeks improved their gait velocity by 25 percent and stride length by 12 percent compared to control groups. A later randomized controlled trial showed that RAS training significantly reduced falls in Parkinson’s patients. A 2018 meta-analysis in Scientific Reports, reviewing 50 studies and nearly 1,900 participants, confirmed that rhythmic cueing improves multiple aspects of gait.
A 2023 review by Koshimori and Thaut goes further, presenting evidence that RAS may influence neural oscillations themselves, not just walking behavior. Researchers are beginning to explore whether rhythmic stimulation could affect tremors and other motor symptoms as well.
Why Music Feels So Good
This raises another question. Why does music feel rewarding in the first place?
Music and Dopamine Release (McGill Study)
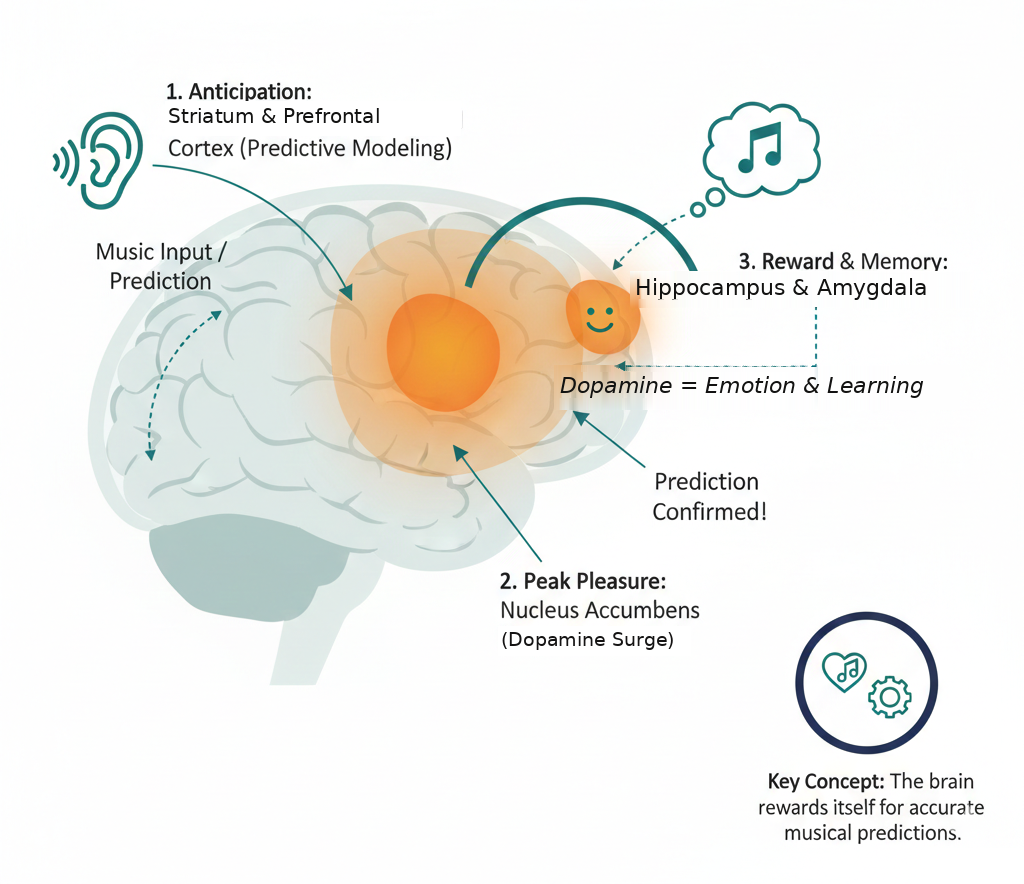
In a 2011 study published in Nature Neuroscience, researchers at McGill University used PET and fMRI imaging to show that the brain releases dopamine during peak moments of musical pleasure. Dopamine is the same neurotransmitter involved in food, social connection, and other rewards. What is especially interesting is that dopamine was released not only during the pleasurable moment itself, but also during the anticipation leading up to it. The brain builds a predictive model of what is coming next in a piece of music and responds when that prediction is fulfilled or artfully violated.
This has implications for therapeutic design. A simple metronome provides a reliable timing cue, but it does not place high demands on prediction. Music with harmonic changes, dynamic shifts, and rhythmic variation engages broader neural networks. EEG research suggests that more complex rhythms recruit premotor and prefrontal regions in addition to auditory and motor areas.
As a jazz musician, this connection feels personal. Jazz is built on syncopation, the intentional displacement of expected beats. Each rhythmic surprise forces the brain to update its predictions. Whether this increased cognitive engagement leads to stronger therapeutic effects remains an open research question, but the hypothesis is consistent with current models of predictive processing.
The Broader Health Context
This research also ties into a larger issue in healthcare. Public health frameworks often estimate that direct clinical care accounts for a relatively small portion of overall health outcomes, while factors such as social connection, environment, and access to stimulation play a much larger role. These influences are commonly referred to as social determinants of health, although their precise contribution varies across populations and conditions.
For older adults in long-term care settings, social isolation is strongly associated with cognitive decline and emotional distress. Music-based programs operate squarely in this space. They do not require prescriptions or insurance authorization, and they are inherently social. A live performance creates shared attention, emotional engagement, and routine.
A 2023 systematic review of randomized controlled trials found measurable cognitive benefits from music therapy in Alzheimer’s patients. A 2024 review in Nature Mental Health examining music therapy in advanced dementia concluded that effective programs need to meet patients where they are in the moment and be integrated into regular routines.
Community-based live music programs are not clinical therapy, but they can complement formal care by providing consistent stimulation and social connection. Research suggests that consistency is an important part of sustained benefit.
What Is Happening Locally
One thing that excites me is how much of this work is happening right here in Austin.
Dell Medical School’s Mulva Clinic for the Neurosciences is a major center for neurological research, including work on brain-computer interfaces, computational neuroscience, and a Comprehensive Memory Center focused on dementia care.
Dell Med has also launched a music program at Dell Seton Medical Center, led by Mark Bernat, a Juilliard-trained double bassist who serves as Director of Music Services. His wife, neuroscience professor and cellist Amy Lee, teaches in UT Austin’s Department of Neuroscience, and the program’s Musical Memories concert series runs through her department.
The broader UT Austin ecosystem, including the Butler School of Music, the Cockrell School of Engineering, and Dell Med, contains many of the elements needed to advance interdisciplinary work connecting music, engineering, and neuroscience.
Where This Is Going
Most music-based interventions today operate in an open-loop format. A therapist selects a tempo or piece of music and observes the patient’s response. Emerging research is exploring closed-loop systems that use wearable sensors to track tremors, heart rate, or gait timing and adjust musical parameters in real time.
Designing such systems is technically demanding. Sensor data are noisy, relevant signals must be extracted quickly, and musical adjustments must occur within roughly 100 to 200 milliseconds to preserve entrainment. Achieving this requires expertise in sensor design, signal processing, neuroscience, and software engineering.
Advances in wearable technology, small-scale computing, and AI music generation are making these systems increasingly feasible. A system that adapts tempo, complexity, and dynamics to a patient’s real-time response could represent a meaningful step toward personalized music-based interventions.
This is one reason I am currently participating in a computational neuroscience program with Prof. V. Srinivasa Chakravarthy at IIT Madras. His lab has spent years building computational models of the basal ganglia to better understand Parkinson’s disease, and he is also the founder of Neurogati, a startup developing AI tools for neurological diagnosis and rehabilitation.
What This Means for Austin Sound Care
We started Austin Sound Care because we believed live music matters to seniors, not just as entertainment, but as meaningful engagement. The research supports that belief. Neural entrainment helps explain how rhythm can reach the brain even in advanced dementia. RAS trials demonstrate measurable clinical effects on movement. Dopamine research explains why music sustains attention and motivation. Public health research highlights the importance of social connection and consistency.
We are not clinicians, and we do not claim to deliver medical treatment. However, we aim to bring something into these communities that neuroscience suggests has real neurological and social value, especially where access to specialized care is limited. Community-based live music programs are unlikely to replace clinical therapy, but they can serve as a complementary component of holistic care.
Further Reading
Jacobsen et al. (2015): "Why musical memory can be preserved in advanced Alzheimer's disease." Published in Brain: PubMed
Thaut et al. (1996): The original RAS study showing 25% gait improvement in Parkinson's patients: PubMed
Thaut et al. (2019): RAS for fall reduction in Parkinson's disease, randomized controlled trial: PubMed
Ghai et al. (2018): Meta-analysis of rhythmic auditory cueing in Parkinson's (50 studies, ~1,900 participants): Nature Scientific Reports
Koshimori & Thaut (2023): RAS as a potential neuromodulator for Parkinson's: PubMed
Salimpoor et al. (2011): Dopamine release during anticipation and experience of musical pleasure: Nature Neuroscience
Bleibel et al. (2023): Music therapy effects on cognitive function in Alzheimer's: Alzheimer's Research & Therapy
McDermott et al. (2024): Music therapy and distress in advanced dementia: Nature Mental Health
Dell Med Music Program: Live music at Dell Seton Medical Center: UT Health Austin
Musical Memories Concert Series: Housed in UT's Department of Neuroscience: UT Neuroscience
Mulva Clinic for the Neurosciences: Dell Med's neuroscience research hub: Dell Medical School